(CMN) or DMERC Information Form (DIF) is required to help document the medical necessity and other coverage criteria for selected DMEPOS items.
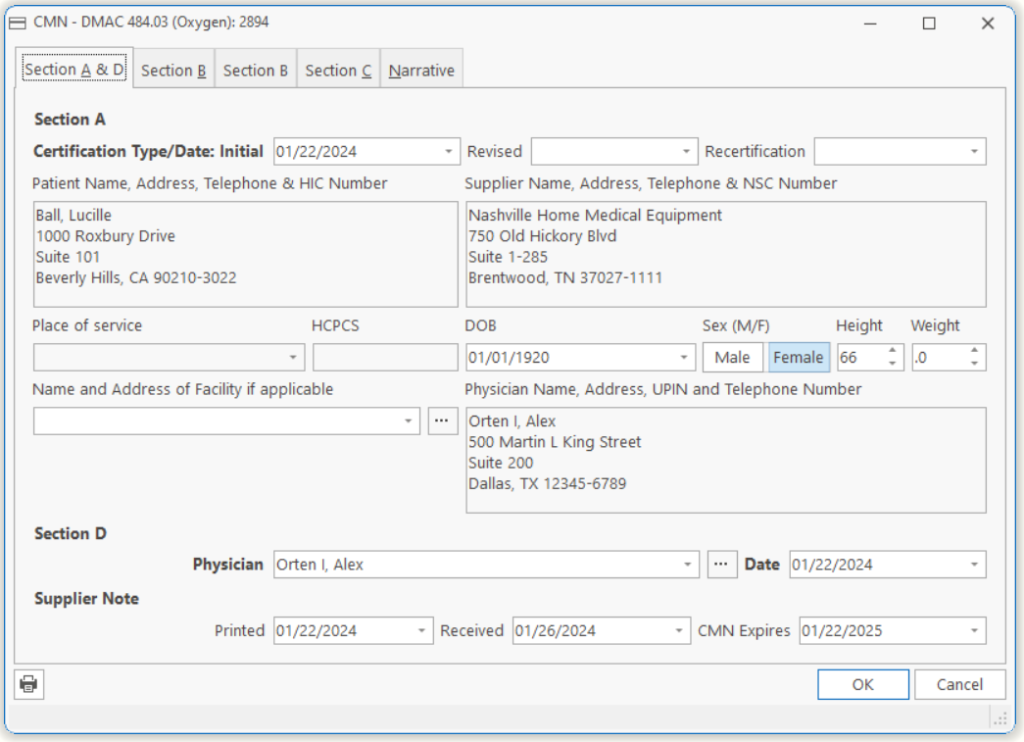
Section A
| Initial | This is the date the CMN was initially submitted. |
| Revised | If the CMN has been changed/updated for some reason, then you will need to put the revised date here. |
| Recertification | If the CMN is being recertified, then put the date of recertification here. |
| Patient Name, Address, Phone, & HIC Number | This is the patient’s name, address, phone, and HIC number as it appears on their insurance card. |
| Supplier Name, Address, Phone, & NSC Number | This is the supplier’s name and address. In other words, the company’s name and address. |
| Place of Service | This is where the equipment will be used. |
| HCPCS | This is the HCPCS code that covers the item associated with the CMN. |
| Name and Address of Facility | If the patient is in a facility, then the name and address will go here. |
| Physician Name, Address, & UPIN Number | This is the physician that wrote the prescription, name, address, phone and UPIN number. |
| In Section A, at least the patient’s name, address, telephone and HIC number, the supplier’s name, address, telephone and NSC number, and the HCPCS codes must be completed by the supplier before the CMN is sent to the physician. The codes which require a CMN/DIF are listed later in this section. These are the codes that should be listed in Section A of the CMN/DIF. Section A of these CMN’s may be completed by the supplier. It is important for the supplier to accurately complete all items in Section A, especially the beneficiary’s name, address and MC number. Include complete supplier information, including the NSC assigned supplier number. Prior Authorizations cannot be completed without this information. The supplier must also include the HCPCS code, complete narrative description, brand name and model number, and all applicable modifiers in the HCPCS Code(s) section. This would include the RR modifier if the equipment were to be rented, and the NU or UE modifier to signify purchase of new or used equipment. |
Section D
| Physician ID | The physician ID of the person who authorized the CMN. |
| Date Signed by Physician | The date the physician signed the CMN. |
| Section D contains the physician’s attestation statement, physician’s signature, and date. The physician who signs the CMN must be the physician who is actively/presently treating the patient. Claims submitted with CMNs lacking a physician signature will be denied. Suppliers billing electronically must indicate presence of the physician’s signature in the usual way. The date in Section D must be the date that the physician signs the CMN. Both the signature and date must be personally entered by the physician and may not be a stamp or other substitute. |
Tell us what you think.
You must be logged in to post a comment.