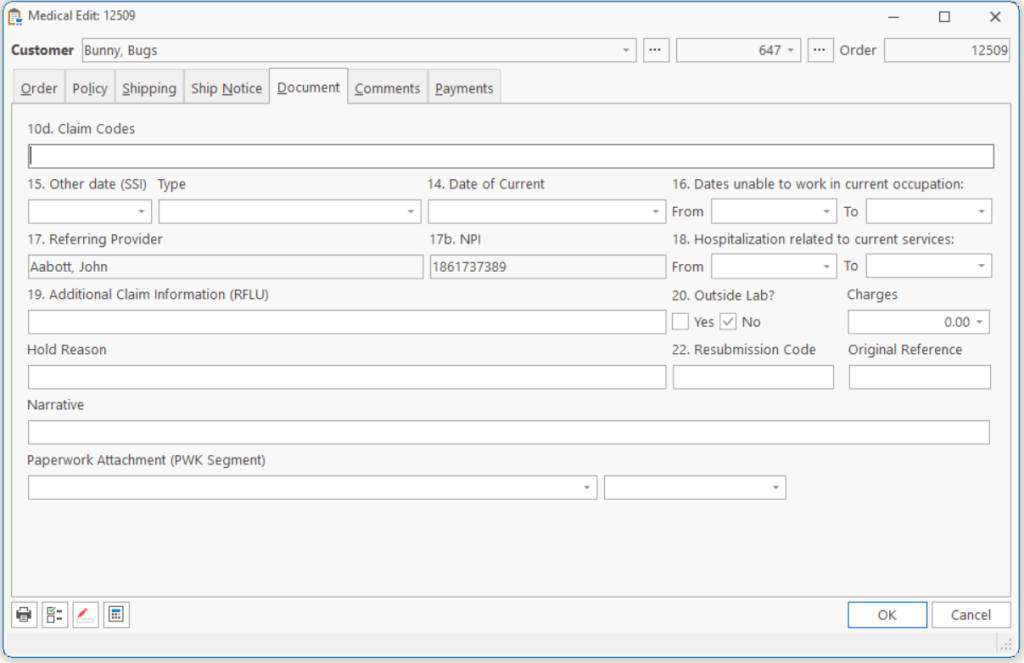
| Date of Current | The date of the current illness, injury or accident. |
| Type | Illness, to indicate illness.
Accident, to indicate accident. Pregnancy, to indicate pregnancy. |
| Date of Similar Illness | The first date patient had the same or a similar illness. |
| Dates unable to work in current occupation | The date range the patient has not been able to work in their current occupation. |
| Referring Physician | The name and NPI of the physician that ordered the equipment or referred the patient. |
| Hospitalization related to services | The dates the patient was hospitalized related to the current services. |
| Reserved for Local Use 19 |
Enter text to fill in Box 19 on CMS-1500 form |
| Outside Lab |
Yes, if there is an outside lab charge on this claim. No, otherwise. |
| Charges | The amount of outside lab charges. |
| Reserved for Local Use 10d | Enter text to fill in Box 10d on CMS-1500 form |
| Hold Reason | The reason you want this Order held. As long as there is something here, the Order/Claim will not be submitted. |
| 22. Resubmission Code | Enter text to fill in Box 22 on CMS-1500 form |
| Original Reference | Enter text to fill in Box 22b on CMS-1500 form |
| Narrative | Enter the text which you would like to attach to the Order to go as the Narrative.Note: Narrative is limited to 80 characters by the ANSI 4010 format. You can have only one per Order, and one on each Line Item. |
| Paperwork Attachment | select the paperwork and type that will be attached to this order. |
Tell us what you think.
You must be logged in to post a comment.